Left Atrium segmentation is a crucial step in cardiac disease diagnosis. Changes in the atrial volume are associated with cardiac diseases such as atrial fibrillation or mitral valve stenosis. Often the segmentation of related LGE-MRI images is carried out manually, a time-consuming and error-prone process. Therefore, we developed a neural network to automatically segment the left atrium from cardiac MRI images.
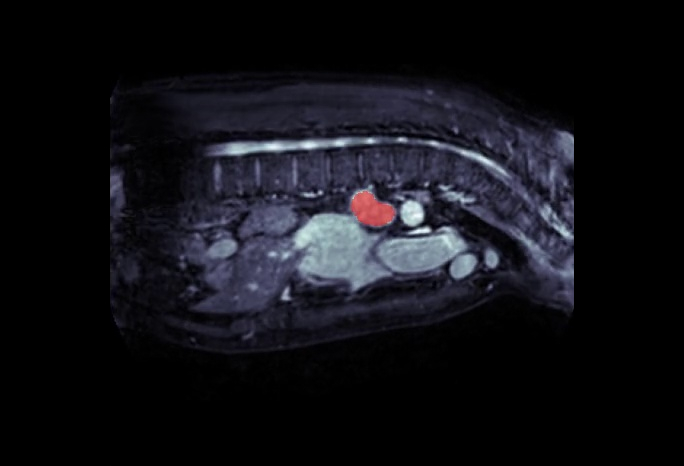
Left Atrium segmentation
Despite improvements, such as the late gadolinium-enhanced MRI (LGE-MRI), manually segmenting the Left Atrium chamber remains time-consuming and error-prone.
In fact, the LA cavity has a complex anatomy, boundaries are blurry and it is relatively small ($73 \pm 14.9 cm^3$). The LA represents a small portion of the overall MRI image with a low signal to background ratio.

When applied to clinical images, deep learning exceeded the human-level accuracy for detecting cancer on cervical images. However, not all the deep learning architectures are equally effective when applied to cardiac imaging. Even within cardiology, each task requires the right blend of image pre-processing, neural network architecture and loss function choice.
Neural network architecture for Left Atrium segmentation
With respect to other approaches, the artificial neural network has the ability to automatically extract features and learn, which makes it particularly suited for image segmentation.
After researching the most promising published approaches, we chose the U-Net, a U-shaped architecture initially developed to segment histological images.
As shown in the image below, we built our U-Net architecture using an encoder and a decoder. The encoder reduces the feature maps by using convolutions + max-pooling and the decoder reconstructs the segmentation mask by using upsampling and convolution. Notably, U-Net uses skip connections between down-sampled feature maps and up-sampled feature maps. Skip connections, shown as dotted lines, perform features-forwarding between the encoding and decoding parts and dramatically improves accuracy.

For this research, we used the Adaptive Moment Estimation (Adam) optimizer, which is a combination of two gradient descent methodologies. Adam is really efficient when working with large problems involving a lot of parameters.
We adopt the Dice score as a loss function, a metric commonly reported in benchmarks and known to favour a correct volume over precise contours.
$$L(\hat{y}, y) = 1 – \frac{2 |\hat{y} \cap y |}{|\hat{y}| + | y |}$$
Finally we used a sigmoid activation function on the prediction with threshold at 0.5.
Results
To test our approach we used 20 MRI scans of the heart including the Ground Truth mask from the Medical Segmentation Decathlon. From these 20 MRI scans, we extracted over 4500 2D MRI slices and labels. We then train-test split the dataset using 16 patients as training data and the remaining 4 for validation.
During image pre-processing, we cropped away non-cardiac regions and background for 32 pixels on each side. We Z-normalized per subject separately and standardized each frame. After training the network for 75 epochs, we achieved a Dice Score of 92.1, an excellent result close to the best-in-class benchmarks. $$ Dice\, Score = 92.1 $$
Further developments
While we are pleased with this result, we believe we could further improve our performance, building on this excellent baseline. For instance, we know that the atrial cavity represents less than 1% of the image volume. The low signal to noise ratio creates a severe class imbalance between the background and the atrial structure signal. Our baseline attempt addressed this class imbalance most simply by cropping away the input image from the centre of the image.
As follow-up work, we may adopt a better approach with two consecutive networks, which we have already successfully tested in other research. For example, we can develop a first CNN to detect the LA, allowing us to crop out the unwanted background before feeding the LA into the segmentation network. Furthermore, we can improve the loss function, by using a metric such as the Hausdorff distance instead of the Dice score.
If interested in these developments, at DEEP AI Lab we can embed our model in an existing application or develop further around the Left Atrium segmentation as suggested above.
Beyond Left Atrium segmentation: other clinical applications
Through a bigger effort, we would be eager to address tougher challenges such as fibrosis or left atrial appendage segmentation. Similarly, we can apply the same LA segmentation approach to the Right Atrium to study the sinoatrial disease.
Furthermore, recent studies revealed the importance of the Right Ventricle (RV) in sustaining hemodynamic stability. While the study of the RV is a relatively young field, we could leverage data sets with expert contour labelling. A multi-stage neural network would then be able to accurately segment the RV alone or the RV/LV simultaneously.
At DEEP AI Lab, we would be happy to help leverage state of the art technology to gain clinically relevant insights in all these areas.
To discuss this or further applications, feel free to contact us.

